
Smart Medical Diagnostic Aid: ResNet50-Based Chest X-Ray Pneumonia Classifier
This project builds a deep learning-based chest X-ray (CXR) classification model to explore how AI can assist preliminary pneumonia screening.
📋 Abstract
This project builds a deep learning-based chest X-ray (CXR) classification model to explore how AI can assist preliminary pneumonia screening.
Addressing the challenge that COVID-19 and pneumonia features are difficult to distinguish visually on X-rays, this project uses MATLAB as the development environment and implements ResNet50 for binary classification tasks (Normal vs. Pneumonia/COVID-19). The model showed relatively high recall on the test set, making it a useful research example for preliminary screening workflows.
🛑 The Problem
During pandemic peaks or in resource-limited regions, radiologists face enormous reading pressure. Traditional manual interpretation has the following pain points:
- Time-Consuming: Physicians need to focus for extended periods examining subtle pulmonary infiltration features.
- Ambiguous Features: Early pneumonia or COVID-19 ground-glass opacities closely resemble normal lung textures, easily causing misdiagnosis.
- Fatigue Errors: Visual fatigue from prolonged work may increase missed diagnosis rates.
🛠️ Technical Deep Dive
1. Data Preprocessing
The dataset contains two classes of chest X-ray images:
- Normal: Clear lung fields with no significant abnormal shadows.
- Pneumonia (Pneumonia/COVID-19): Lungs showing patchy shadows or consolidation.
To improve model generalization, I standardized the original images and resized them to ResNet50’s required input dimensions ($224 \times 224$ pixels).
 Figure 1: Normal chest X-ray image with clear lung fields.
Figure 1: Normal chest X-ray image with clear lung fields.
 Figure 2: Chest X-ray image showing pneumonia with visible fuzzy shadows in the lungs.
Figure 2: Chest X-ray image showing pneumonia with visible fuzzy shadows in the lungs.
2. Core Architecture: ResNet50 and Residual Learning
Traditional Convolutional Neural Networks (CNN) often encounter vanishing gradient or gradient explosion problems when layers deepen, causing training performance to actually decrease.
To train a network as deep as 50 layers, I adopted the ResNet (Residual Network) architecture. Its core innovation is introducing “Shortcut Connections”.
Assuming the input to a neural network layer is $x$ and the desired feature mapping is $H(x)$. ResNet doesn’t directly learn $H(x)$, but learns the residual function $F(x) = H(x) - x$. The final output is:
$$y = F(x, {W_i}) + x$$
- $F(x, {W_i})$: Residual Mapping, the change the network layers need to learn.
- $x$: Identity Mapping, directly passing input information to output.
This $y = F(x) + x$ structure ensures that even in extremely deep networks, gradients can flow back directly through this “highway” of $x$, allowing the model to effectively capture extremely subtle pathological features in X-ray images.
3. Training Strategy
Training was performed using MATLAB’s Deep Learning Toolbox.
- Optimizer: SGDM (Stochastic Gradient Descent with Momentum)
- Loss Function: Cross Entropy Loss (Binary Cross Entropy)
📊 Results & Analysis
Based on the test set Confusion Matrix, we quantitatively evaluated the model’s performance:
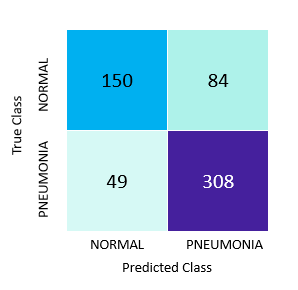 Figure 3: Test set Confusion Matrix.
Figure 3: Test set Confusion Matrix.
1. Confusion Matrix Data Interpretation
Total test set samples: $N = 591$ images
- True Positive (TP, Successfully predicted pneumonia): 308 images
- True Negative (TN, Successfully predicted normal): 150 images
- False Positive (FP, Incorrectly classified as pneumonia): 84 images
- False Negative (FN, Missed pneumonia): 49 images
2. Key Metrics Calculation
Accuracy: $$Accuracy = \frac{TP + TN}{Total} = \frac{308 + 150}{591} \approx 77.5%$$ The model’s overall correct judgment rate is approximately 77.5%.
Recall / Sensitivity: $$Recall = \frac{TP}{TP + FN} = \frac{308}{308 + 49} \approx 86.3%$$ Recall is an important metric in medical-image screening. Among all actual pneumonia samples, the model identified 86.3% of cases, suggesting some value for reducing missed positives in a screening-oriented workflow.
Precision: $$Precision = \frac{TP}{TP + FP} = \frac{308}{308 + 84} \approx 78.6%$$ Among cases the model classified as pneumonia, 78.6% were confirmed. Although some normal individuals were misclassified as pneumonia (84 false positive cases), in medical screening contexts, “better to over-diagnose (False Positive) than to miss (False Negative)” is an acceptable trade-off.
Conclusion
This project implemented automated chest X-ray classification using the ResNet50 architecture. On the test set, the model reached 86.3% recall, which makes it a research prototype for flagging potentially high-risk images. Practical medical use would still require larger datasets, clinical validation, and integration with professional radiology workflows.